Weight Loss and Sleep Apnea: How BMI Directly Impacts CPAP Pressure Needs
 Dec, 5 2025
Dec, 5 2025
How Your Weight Changes What Your CPAP Machine Needs
If you’re using a CPAP machine for sleep apnea and you’ve noticed your mask feels tighter, your pressure settings seem too high, or you’re gaining weight despite feeling better at night - you’re not alone. The link between your body mass index (BMI) and your CPAP needs isn’t just theoretical. It’s measurable, predictable, and deeply personal.
For every 1-point drop in BMI, your apnea-hypopnea index (AHI) - the measure of how many times you stop breathing each hour - drops by about 6.2%. That means if you lose 7 pounds, you can expect a 7% reduction in breathing pauses during sleep. For someone with a BMI of 38, losing 20 pounds could cut their AHI by nearly half. In some cases, that’s enough to stop needing CPAP altogether.
Why Higher BMI Means Higher CPAP Pressure
CPAP machines work by pushing a steady stream of air through your airway to keep it open. But that air pressure isn’t one-size-fits-all. The more fat you carry - especially around your neck, chest, and abdomen - the more pressure you need to keep your airway from collapsing.
Studies show that for every 1-point increase in BMI, CPAP pressure needs go up by about 0.5 cm H₂O on average. So if you’re at a BMI of 35, you might need 14 cm H₂O. At a BMI of 40, that could jump to 18 cm H₂O or higher. That’s not just a number - it’s a physical challenge. Higher pressure means more noise, more dryness, more mask leaks, and more discomfort. It’s no surprise that people with BMI over 35 report significantly worse CPAP adherence than those with lower BMIs.
Neck circumference matters, too. A neck size over 17 inches in men or 16 inches in women is a strong red flag for obstructive sleep apnea. It’s not just about overall weight - it’s about where the fat is stored. Fat around the neck squeezes the airway like a collar. That’s why two people with the same BMI can have very different CPAP needs.
The Paradox: CPAP Can Make You Gain Weight
Here’s the twist: treating sleep apnea with CPAP can sometimes make weight loss harder.
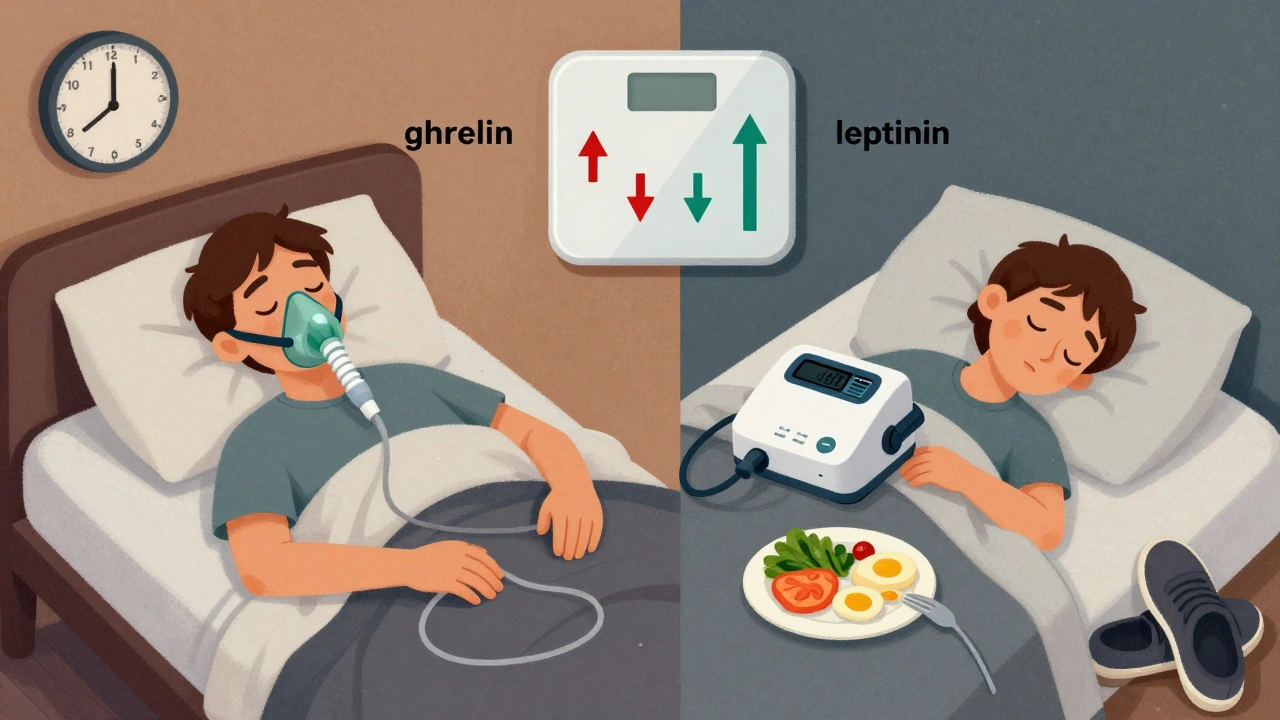
Multiple studies have found that after starting CPAP, people tend to gain a little weight - on average, about 2.6 pounds over six months. Why? Because when you finally sleep well, your body changes. Your ghrelin (the hunger hormone) goes up. Your leptin (the fullness hormone) goes down. Your metabolism slows slightly. You feel less tired during the day - but instead of using that energy to move, many people just eat more.
One study of 63 patients found that after starting CPAP, people reported eating 287 extra calories a day. That’s like adding a bagel and a banana to your lunch. Over time, that adds up. And if you’re only using CPAP 4 hours a night - not the recommended 5+ - the metabolic disruption is worse. Consistent use cuts the weight gain risk in half.
But here’s the good news: CPAP doesn’t cause weight gain because it’s broken. It’s because it works. When your body stops fighting for air every night, it stops storing fat as a survival mechanism. You just need to match that new energy with better habits.
Weight Loss Can Reduce - or Eliminate - Your CPAP Needs
There’s a clear path out of high-pressure CPAP: lose weight. And you don’t need to lose 100 pounds to see results.
Research shows that losing just 5-10% of your body weight leads to major improvements in sleep apnea. For someone weighing 200 pounds, that’s 10-20 pounds. That’s enough to drop your CPAP pressure by 2-3 cm H₂O. In one survey of 1,200 users, 74% of those who lost 10% of their body weight were able to lower their CPAP pressure. And 31% of mild sleep apnea patients stopped needing CPAP entirely.
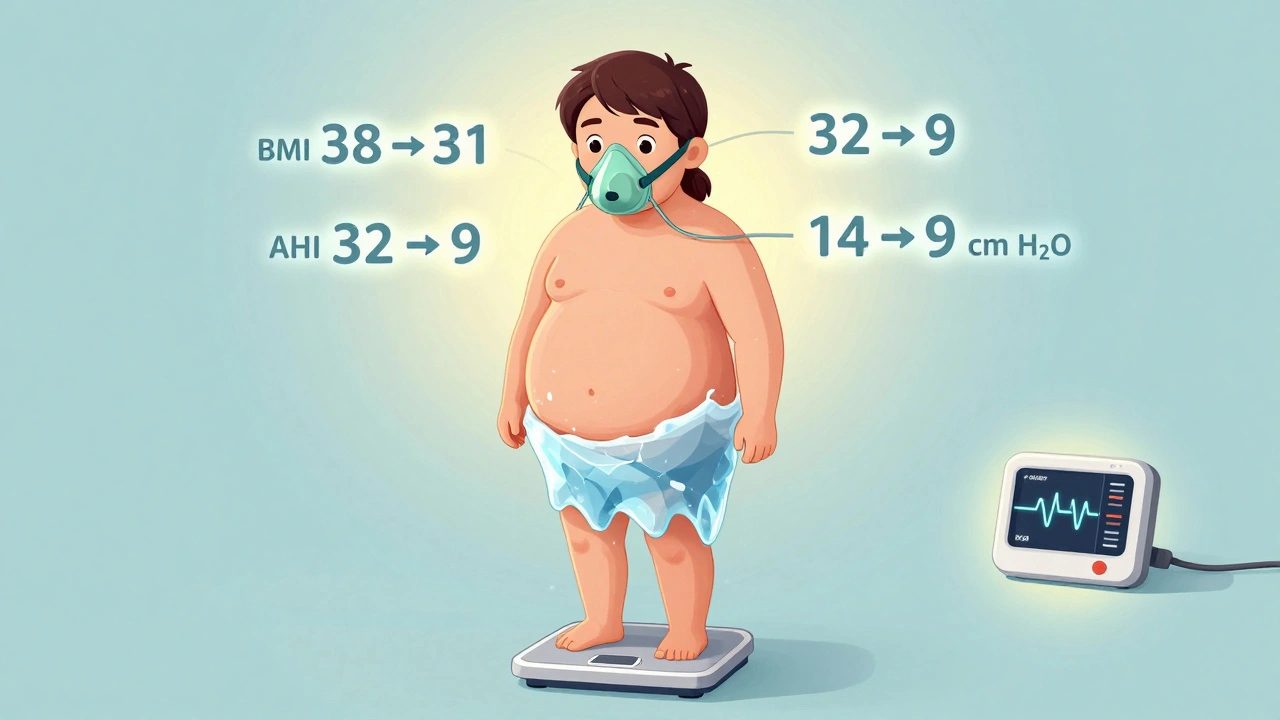
One Reddit user, u/SleepWarrior42, lost 45 pounds - going from BMI 38 to 31. His AHI dropped from 32 to 9. His CPAP pressure went from 14 to 9 cm H₂O. He now only uses it when sleeping on his back.
For people with severe obesity (BMI ≥40), bariatric surgery is the most effective solution. Studies show 78% of patients see their sleep apnea resolve within a year after gastric bypass. Even lifestyle changes - diet, exercise, and sleep-focused coaching - work better when they’re coordinated. A 2021 trial found that patients who worked with a team of sleep doctors, dietitians, and obesity specialists lost 42% more weight than those who just got general advice.
What You Should Do - Step by Step
If you’re on CPAP and your BMI is above 25, here’s what to do next:
- Get your current AHI and BMI recorded. Your sleep doctor should have these numbers. If not, ask for them.
- Set a realistic weight loss goal. Aim for 5-10% of your body weight. That’s enough to make a measurable difference.
- Track your CPAP usage. Use the app that comes with your machine. Aim for 6+ hours a night. Inconsistent use worsens metabolic issues.
- Get support. Don’t try to do this alone. Ask your doctor for a referral to a registered dietitian who understands sleep apnea. Look for an obesity medicine specialist - they’re trained in this exact intersection.
- Re-test your sleep after losing 10% of your weight. Your doctor should schedule a follow-up sleep study. You might be able to lower your pressure - or even stop CPAP.
Many people think CPAP is a lifelong sentence. But for a lot of people, it’s a bridge - not a life sentence. Weight loss doesn’t just make CPAP easier. It can make it unnecessary.

The New Tech Helping You Connect Weight and Sleep
Device makers are catching up. ResMed’s AirSense 11 AutoSet for Her now has algorithms calibrated specifically for people with BMI over 35. Philips’ DreamStation 3, released in late 2023, can track your weight changes and auto-adjust pressure settings - if you input the data.
These aren’t magic fixes. But they’re signs that the medical world is finally recognizing that sleep apnea isn’t just a breathing problem - it’s a metabolic one. And treating it means treating the whole body.
Insurance and Access: What You Can Do
Getting help isn’t always easy. Medicare requires an AHI over 15 (or over 5 with other health issues) to cover CPAP. But weight loss programs? Only 41% of private insurers cover FDA-approved weight-loss medications. That’s changing slowly. More clinics are now offering integrated sleep and weight programs - especially in academic medical centers.
If your doctor won’t refer you to a dietitian or obesity specialist, ask for a second opinion. You’re not asking for a favor - you’re asking for standard care. The American Academy of Sleep Medicine updated its 2023 guidelines to say every sleep apnea patient should get weight management counseling. That’s not optional. It’s part of the treatment plan.
Final Thought: It’s Not About Willpower - It’s About Biology
Sleep apnea and obesity feed each other. Poor sleep makes you hungrier. Extra weight makes your airway collapse. CPAP fixes the breathing - but not the hunger. And that’s why so many people feel stuck.
But here’s the truth: you’re not failing because you’re lazy. You’re struggling because your body’s chemistry is working against you. The solution isn’t just to push harder. It’s to work smarter - with the right tools, the right support, and the right expectations.
Losing weight won’t just help your CPAP. It’ll help your heart, your blood sugar, your energy, and your life. And the best part? You don’t have to lose it all to start seeing results. Every pound counts. Every night of better sleep adds up.
Can losing weight eliminate the need for CPAP?
Yes - especially for people with mild to moderate obstructive sleep apnea. Losing 5-10% of your body weight can reduce your AHI enough to stop needing CPAP. One study found 31% of mild OSA patients discontinued CPAP after significant weight loss. Always follow up with a sleep study before stopping treatment.
Why does CPAP sometimes cause weight gain?
CPAP improves sleep, which changes your hormones. Ghrelin (hunger) increases, leptin (fullness) decreases, and your metabolism may slow slightly. Many people also eat more because they have more energy during the day - but don’t channel it into activity. Consistent use (6+ hours/night) reduces this effect.
How much weight do I need to lose to see results?
Losing just 5-10% of your body weight leads to measurable improvements. For example, a 200-pound person losing 10-20 pounds can reduce their AHI by 30-50% and lower CPAP pressure by 2-3 cm H₂O. Even small losses reduce neck fat and improve airway openness.
Does CPAP pressure automatically adjust with weight loss?
Most standard CPAP machines don’t auto-adjust based on weight. You need to manually update your weight in the device settings (if supported) or get a new sleep study to have your pressure re-titrated. Newer models like the Philips DreamStation 3 can track weight changes and adjust pressure - but only if you enter the data.
Is bariatric surgery worth it for sleep apnea?
For people with severe obesity (BMI ≥40), yes - it’s the most effective treatment. Studies show 78% of patients see their sleep apnea resolve within a year after gastric bypass. Lifestyle changes alone resolve it in about 37% of cases. Surgery isn’t for everyone, but for those with BMI over 40, it often eliminates the need for CPAP completely.
What’s the best way to lose weight while using CPAP?
Work with a team: a sleep specialist, a registered dietitian, and an obesity medicine doctor. Studies show patients with coordinated care lose 42% more weight than those getting standard advice. Focus on consistent CPAP use (6+ hours/night), protein-rich meals, and gentle movement - even walking 10 minutes after meals helps. Avoid crash diets - they worsen sleep quality.
Kenny Pakade
December 7, 2025 AT 02:39brenda olvera
December 8, 2025 AT 21:27olive ashley
December 10, 2025 AT 16:09joanne humphreys
December 12, 2025 AT 13:33Nigel ntini
December 14, 2025 AT 05:02Priya Ranjan
December 16, 2025 AT 03:45Ashish Vazirani
December 16, 2025 AT 22:11Dan Cole
December 18, 2025 AT 10:55Max Manoles
December 20, 2025 AT 09:07Katie O'Connell
December 22, 2025 AT 04:42