Urate Targets in Gout: How Allopurinol and Febuxostat Work to Reach Treatment Goals
 Dec, 7 2025
Dec, 7 2025
Most people think gout is just about painful toes and swollen joints. But the real battle happens in your blood - at the level of urate. If your serum urate stays too high, crystals keep forming, flares keep coming, and tophi keep growing. The goal isn’t just to calm a flare. It’s to drive urate levels low enough to dissolve those crystals for good. That’s where allopurinol and febuxostat come in - and why hitting the right urate target isn’t optional. It’s the foundation of real, lasting control.
What Urate Target Should You Be Shooting For?
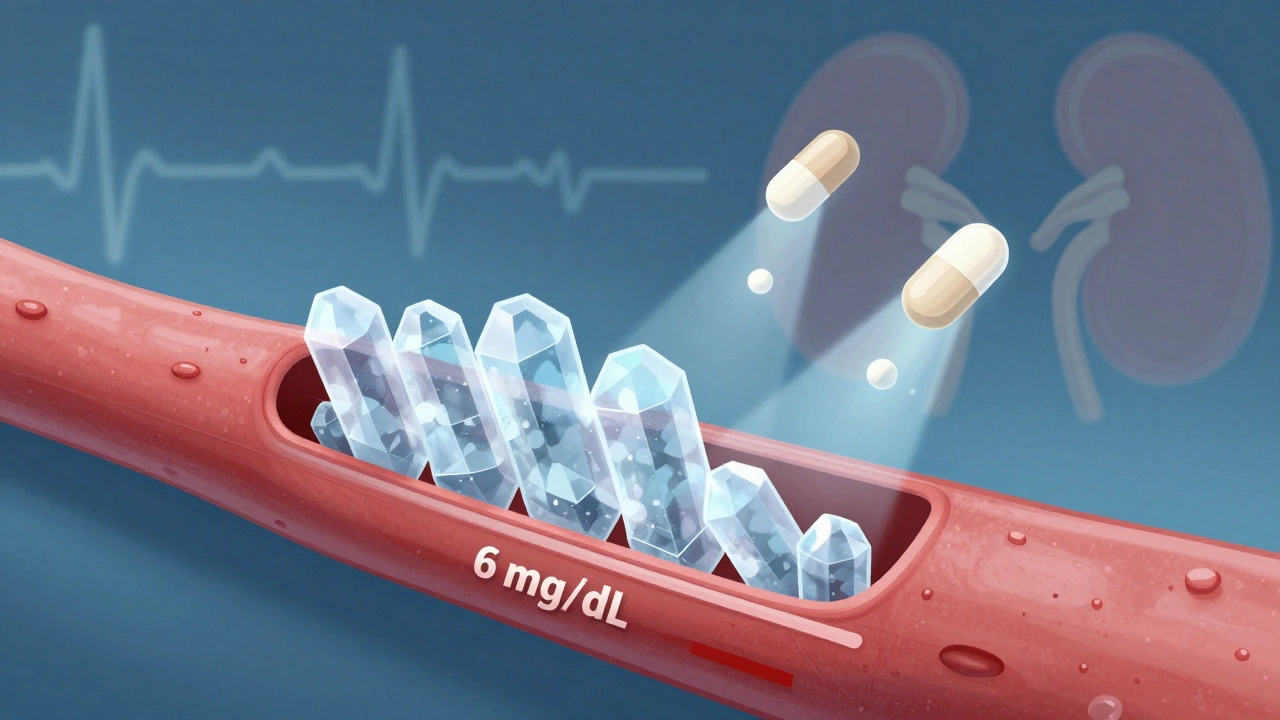
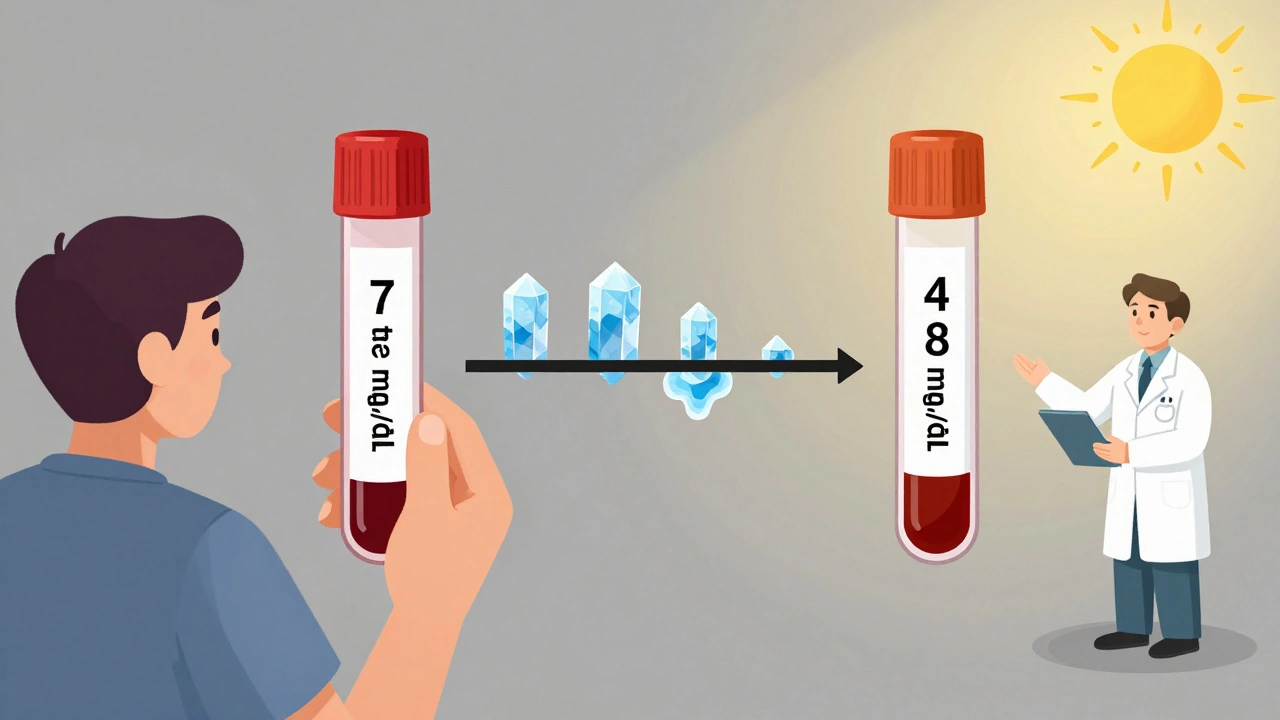
The science is clear: if your serum urate stays above 6 mg/dL (360 micromol/L), your body keeps making monosodium urate crystals. These crystals are what trigger flares. But if you drop below that number, your body starts dissolving them. That’s the magic line. For most people with gout, the target is simple: below 6 mg/dL.
But if you’ve got tophi - those visible lumps under your skin - or joint damage shown on X-rays, or flares that won’t quit even on standard treatment, you need to go lower. That’s where the 5 mg/dL (300 micromol/L) target comes in. Studies show people who hit this lower number lose tophi faster and stay flare-free longer. One 2023 study found 89% of patients with tophi saw major shrinkage when urate stayed below 0.30 mmol/L, compared to just 72% at the higher target.
And here’s what no one tells you: you don’t want to go too low. Below 3 mg/dL (180 micromol/L), there’s no extra benefit - and some concern about unknown risks. So the goal isn’t to crush urate. It’s to hold it steady in the sweet spot: low enough to dissolve crystals, but not so low it causes new problems.
Allopurinol: The First-Line Workhorse
Allopurinol has been around since the 1960s. It’s cheap - often under $10 a month. It blocks the enzyme that makes uric acid, so your body produces less. And it’s still the first choice for most guidelines, including the 2020 American College of Rheumatology (ACR) and 2023 EULAR recommendations.
But here’s the catch: most people start too low. Doctors often prescribe 100 mg a day. That’s fine for someone with mild gout and normal kidneys. But for most patients, it’s not enough. Real-world data from New Zealand shows that 30-50% of people need more than 300 mg daily to hit their target. Some need 600 mg, even 800 mg. And that’s okay - if you’re monitored.
The key is titration. Start at 100 mg (or 50 mg if you have kidney issues). Check your serum urate in 4-6 weeks. If you’re still above 6 mg/dL, bump the dose up by 50-100 mg. Do this every 3-4 weeks until you hit your target. Don’t just stay on the starter dose. That’s why so many people fail - they’re on a dose that’s too low for too long.
There’s one big warning: allopurinol can cause a rare but serious skin reaction called allopurinol hypersensitivity syndrome. It’s rare - 0.1-0.4% of users - but 25 times more likely if you carry the HLA-B*5801 gene. That’s why testing for this gene is recommended for people of Asian descent or those with kidney disease. But even without testing, if you get a rash, fever, or blisters, stop it immediately and call your doctor.
Febuxostat: The Alternative for Tough Cases
Febuxostat works the same way - it blocks uric acid production. But it’s not broken down by the kidneys. That makes it a better option if you have moderate to severe kidney disease. A 2023 meta-analysis showed febuxostat helped 15% more patients hit their urate target than allopurinol in those with CKD stage 3 or worse.
It’s also useful if you’ve tried allopurinol and couldn’t get to your target, even at high doses. Or if you had a bad reaction to it. In New Zealand, febuxostat use has risen steadily since 2020, especially among Māori and Pacific patients who often have more severe gout and higher rates of kidney problems.
Febuxostat starts at 40 mg daily. If your urate is still above target after 2 months, you can go up to 80 mg. Unlike allopurinol, you don’t need to adjust the dose for kidney disease - it’s safe at 40 or 80 mg even if your kidneys aren’t perfect.
But it’s not without risks. The FDA added a black box warning in 2019 after a trial showed a slightly higher risk of heart-related death compared to allopurinol. That doesn’t mean you can’t use it - it means you need to weigh the risks. If you have heart disease, or a history of stroke or heart attack, allopurinol is still safer. If you’re otherwise healthy and need better urate control, febuxostat is a strong second option.
Why Most People Fail to Hit Their Target
Here’s the hard truth: only about 42% of gout patients in New Zealand reach their urate target within a year. Why? Three big reasons.
First, doctors don’t monitor enough. The guidelines say check serum urate every 4-6 weeks during titration. But U.S. Medicare data shows only 54% of patients get tested that often. If you don’t measure, you don’t know if you’re on the right dose. And if you don’t adjust, you won’t reach your target.
Second, patients stop because of flares. When you start allopurinol or febuxostat, you might get more flares at first. It’s not the drug failing - it’s the crystals dissolving and stirring up inflammation. This is called the “flare paradox.” It’s normal. The solution? Start with a low-dose colchicine or NSAID for the first 6 months. Don’t stop your ULT because of a flare. That’s how tophi grow.
Third, there’s a lack of education. A 2023 survey of gout patients found 62% said their doctor never explained how to titrate the dose. Many think, “I’m on medicine, I’m fine.” They don’t realize they need to keep adjusting until their blood level is right. One patient in Auckland told me, “I was on 300 mg for two years. My doctor never checked my urate. I had three flares a year. Then I switched to a pharmacist-led clinic - they upped me to 600 mg. No flares in 18 months.”
What About Asymptomatic High Urate?
If your urate is 7 mg/dL but you’ve never had a gout flare? Don’t start medication. The 2020 ACR guideline is clear: treat gout, not high numbers. There’s no proof that lowering urate in someone with no symptoms prevents future flares. And there’s no benefit to exposing someone to drug risks for no reason.
Focus on lifestyle: reduce alcohol (especially beer), cut back on sugary drinks, lose weight if needed, avoid organ meats. But don’t start allopurinol just because your blood test says “high.” Wait for the first flare. Then - and only then - start the long game of urate control.
What’s New in 2025?
The field is moving fast. In 2024, the ACR updated its quality measures to say: successful treatment means two consecutive urate readings below 6 mg/dL, at least 30 days apart. That’s a big step. It stops people from claiming success after one lucky reading.
And now, for severe gout, EULAR recommends “treat-to-dissolve.” That means using dual-energy CT scans to confirm tophi are actually shrinking before you relax your target. It’s not routine yet - but it’s coming.
There’s also new research on genetics. The GOUT-PRO study found that testing for ABCG2 and SLC22A12 gene variants helped predict who responds to allopurinol. Patients who got genotype-guided dosing reached targets in 83% of cases - up from 61%. This isn’t standard yet, but it’s the future.
And a new drug, verinurad, is in phase 3 trials. It’s a uricosuric - it helps your kidneys flush out more urate. It might let people hit targets with lower doses, fewer side effects. Results are expected in late 2025.
What Should You Do Right Now?
If you have gout and are on allopurinol or febuxostat, ask yourself these questions:
- Have I had my serum urate checked in the last 3 months?
- Do I know what my target is - 6 mg/dL or 5 mg/dL?
- Am I on the highest dose my doctor thinks is safe for me?
- Am I taking a low-dose anti-inflammatory to prevent flares during the first 6 months?
If you answered no to any of these, talk to your doctor or pharmacist. Don’t wait for the next flare. Urate targets aren’t a suggestion. They’re the only way to stop gout from getting worse. And with the right dose, the right monitoring, and the right patience - you can get there.
Taya Rtichsheva
December 9, 2025 AT 00:33Carina M
December 10, 2025 AT 09:54William Umstattd
December 10, 2025 AT 14:14Angela R. Cartes
December 11, 2025 AT 03:21Lisa Whitesel
December 12, 2025 AT 06:05Larry Lieberman
December 13, 2025 AT 12:50Courtney Black
December 13, 2025 AT 17:58Anna Roh
December 14, 2025 AT 17:46om guru
December 14, 2025 AT 23:44