Oral Appliance Therapy for Snoring: How Mandibular Advancement Works
 May, 1 2026
May, 1 2026
Imagine waking up to a quiet bedroom instead of the roar of your partner’s snoring. For millions of people, this isn’t just a luxury-it’s a medical necessity. Oral Appliance Therapy (OAT), specifically using Mandibular Advancement Devices, has emerged as one of the most effective non-invasive solutions for primary snoring and mild-to-moderate obstructive sleep apnea. Unlike bulky machines that require electricity and masks, these custom-fitted dental devices work by gently pulling your lower jaw forward while you sleep. This simple mechanical action keeps your airway open, reducing the vibration that causes snoring. If you’ve tried nasal strips or positional pillows without success, OAT might be the missing piece in your sleep puzzle.
How Mandibular Advancement Devices Actually Work
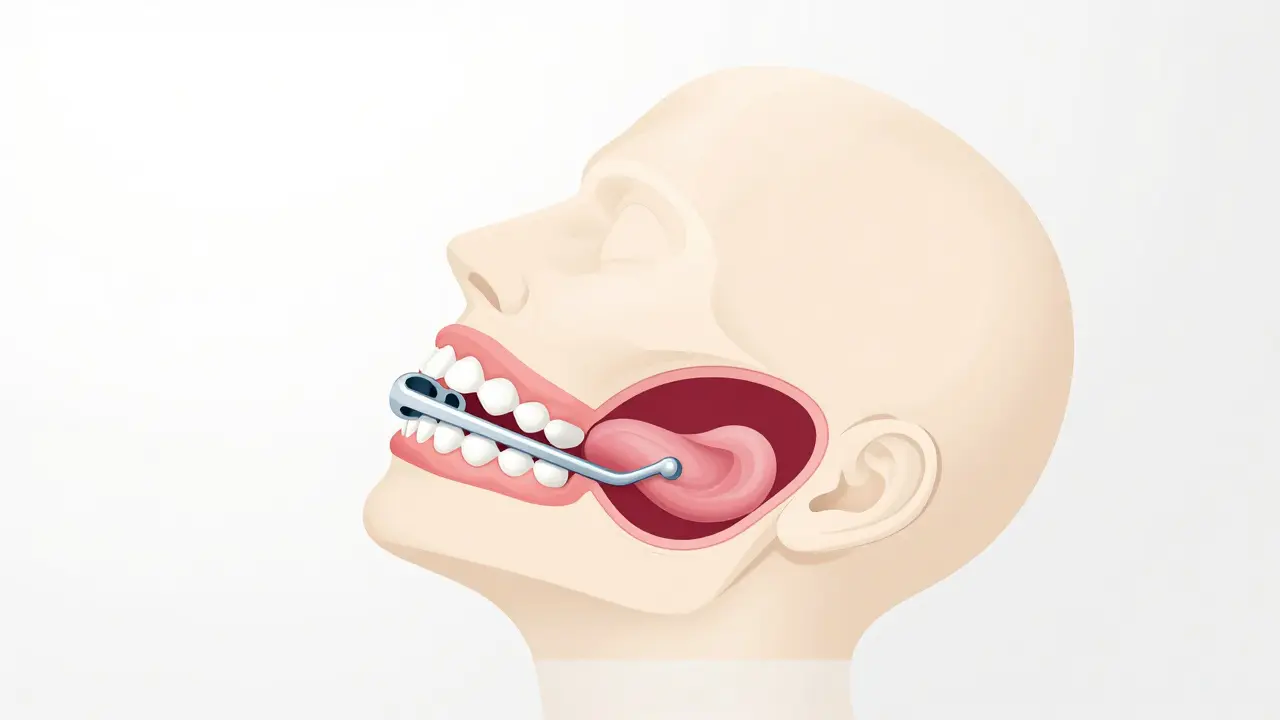
To understand why these devices are so effective, you need to look at basic anatomy. When you lie down, gravity pulls the soft tissues in your throat backward. In many people, this narrows the airway enough to cause turbulence-what we hear as snoring-or even complete blockage, known as obstructive sleep apnea. A Mandibular Advancement Device (MAD) works like a seatbelt for your tongue and soft palate. By holding your lower jaw (mandible) slightly forward, it pulls the attached muscles tight, preventing them from collapsing into your airway.
The science behind this is well-established. Dr. Nobuyoshi Kato’s landmark study in 1999 showed that even small amounts of jaw protrusion-just 2mm to 6mm-significantly lowered apnea-hypopnea index (AHI) values. Today, clinical guidelines confirm that optimal snoring reduction often occurs at about 75% of your maximum comfortable jaw protrusion, which usually translates to 8-10mm of movement. It’s not about forcing your jaw to its absolute limit; it’s about finding the "sweet spot" where your airway stays open but your joints remain comfortable.
Custom Prescription vs. Over-the-Counter Options
Not all mouthpieces are created equal. You’ll find two main categories on the market: custom prescription devices and over-the-counter (OTC) boil-and-bite models. The difference lies in precision, material, and efficacy.
| Feature | Custom Prescription MAD | Over-the-Counter (OTC) |
|---|---|---|
| Efficacy | 72-85% snoring reduction | 45-50% snoring reduction |
| Material | Semi-rigid acrylic, titanium connectors | Thermoplastic polymer |
| Titration | Adjustable in 0.5-1.0mm increments | Fixed advancement (3-5mm) |
| Cost | $1,800 - $2,500 | $99 - $200 |
| Fabrication | Dental impressions or 3D scans | Boil-and-bite molding at home |
Custom devices, such as the SomnoDent MAS or TAP 3, are built by dental laboratories using precise impressions of your teeth. They allow for fine-tuned adjustments, meaning your dentist can gradually increase the jaw position over weeks to maximize comfort and effectiveness. OTC options like Zyppah or Good Morning Snore Solution are cheaper and easier to get, but they lack this precision. A 2015 meta-analysis found that custom titratable devices achieved significantly better results than non-custom alternatives. If snoring is severely impacting your life or your partner’s health, investing in a custom device is usually worth the extra cost.
Who Is a Good Candidate for Oral Appliance Therapy?
OAT isn’t a one-size-fits-all solution. While it helps many people, certain anatomical and health factors determine whether you’ll benefit. Generally, you’re a good candidate if:
- You have primary snoring without severe sleep apnea.
- You have mild-to-moderate obstructive sleep apnea (OSA) and cannot tolerate CPAP therapy.
- You have at least 6-8 natural teeth per arch to anchor the device.
- You do not have severe temporomandibular joint (TMJ) disorders or advanced periodontal disease.
Conversely, OAT may fail if you have severe anatomical obstructions, such as a very large tongue base or significant velopharyngeal collapse. Studies show failure rates reach nearly 40% in patients with Mallampati class IV airways (where you can’t see your uvula when opening your mouth wide). In these cases, surgery or CPAP might be more appropriate. Always start with a sleep study-either polysomnography or a home sleep test-to rule out severe OSA before committing to an oral appliance.
The Adjustment Period: What to Expect
Putting a foreign object in your mouth every night takes getting used to. Most users experience a learning curve of 10-14 days. During this time, you might notice increased salivation, mild jaw soreness, or tooth discomfort. These side effects are normal and typically subside within four weeks. Here’s how to make the transition smoother:
- Start Slow: Wear the device during the day for short periods to acclimatize your muscles.
- Follow Titration Protocols: Don’t jump straight to maximum advancement. Increase the jaw position by 1mm every 3-5 days as directed by your specialist.
- Use Warm Water: If your device feels stiff, soaking it in warm water can soften the material slightly, making insertion easier.
- Communicate with Your Dentist: If pain persists beyond four weeks, your device may need adjustment.
Patience is key. Research shows that 76.4% of users achieve consistent nightly use by the 30-day mark once they get past the initial hump.
Long-Term Safety and Dental Side Effects
One of the biggest concerns with long-term OAT use is the potential for dental changes. Because the device holds your jaw in a forward position, it can alter how your teeth fit together (occlusion) over time. Dr. Avram Gold from SUNY warns that approximately 25% of long-term users develop irreversible occlusal changes that may require orthodontic correction. Other common side effects include:
- Morning jaw pain (reported by 68% of new users initially).
- Excessive drooling.
- Tooth sensitivity or loose teeth in rare cases.
To mitigate these risks, regular dental check-ups every six months are crucial. Your dentist will monitor your bite and adjust the device if necessary. Despite these concerns, the benefit-risk profile remains favorable for properly selected patients. The relief from chronic snoring and improved sleep quality often outweighs the manageable dental side effects.

Cost and Insurance Coverage
Affordability is a major hurdle for many patients. Custom MADs typically cost between $1,800 and $2,500. Unfortunately, insurance coverage varies widely. According to 2023 data, only 38% of U.S. commercial insurance plans cover MADs for primary snoring. However, if you have a diagnosed sleep apnea, coverage is more likely. Some plans consider it a medical necessity rather than a dental procedure. Before proceeding, call your insurer to ask specifically about "sleep-related breathing disorder" coverage. If you’re paying out-of-pocket, ask your provider about payment plans or financing options.
Future Innovations in Sleep Technology
The field of dental sleep medicine is evolving rapidly. Newer devices like the SomnoDent EVO 3 now come with integrated sensors that track your snoring levels and send data to a smartphone app. This real-time feedback allows dentists to fine-tune the device remotely, ensuring you’re getting the optimal therapeutic effect. Looking ahead, AI-driven titration algorithms and genetic markers may soon help predict the ideal device design for each individual patient, making treatment more personalized and effective.
Does an oral appliance cure snoring permanently?
No, oral appliances do not provide a permanent cure. They manage snoring while you wear them. If you stop using the device, snoring typically returns within 48 hours. Consistent nightly use is required to maintain benefits.
Can I buy a mandibular advancement device online without a dentist?
Yes, you can buy over-the-counter devices online. However, these are less effective and carry higher risks of improper fit, which can lead to jaw pain or dental damage. Custom devices prescribed by a dental sleep specialist offer better safety and efficacy.
How long does it take to get used to wearing a MAD?
Most people adapt within 10 to 14 days. Initial side effects like dry mouth, jaw soreness, and excess saliva are common but usually resolve within four weeks. Starting with daytime wear can speed up the adjustment process.
Is oral appliance therapy better than CPAP?
It depends on your condition. CPAP is more effective at completely stopping apnea events, especially in severe cases. However, MADs have much higher adherence rates because they are quieter, portable, and more comfortable. For primary snoring or mild OSA, MADs are often preferred due to ease of use.
Will my teeth move back to normal after removing the device?
Minor shifts may reverse, but long-term use can cause permanent changes in your bite (occlusion). Regular monitoring by a dentist is essential to prevent irreversible dental issues. Some users may need orthodontic treatment later in life.