Hypertensive Retinopathy: How High Blood Pressure Damages Your Eyes
 Apr, 7 2026
Apr, 7 2026
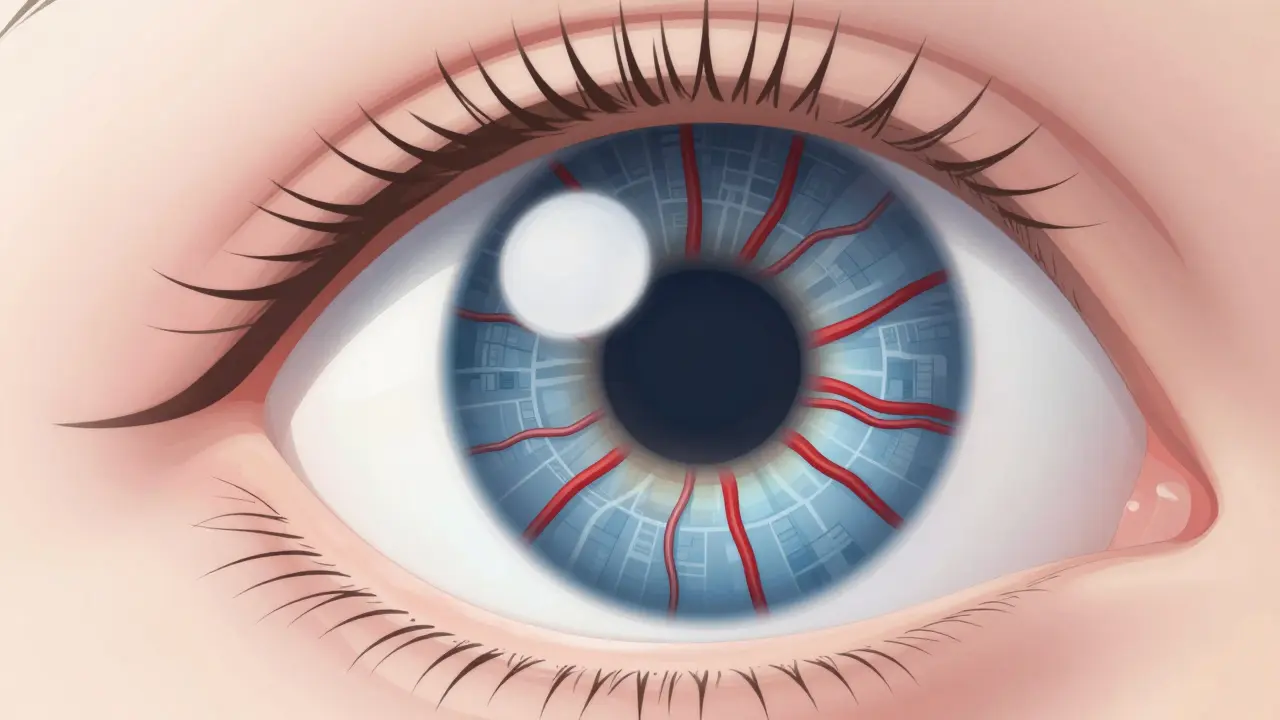
Imagine waking up and seeing dark spots in your central vision or a strange "curtain" falling across your field of view. For many people, these frightening symptoms aren't caused by a direct eye injury, but by a silent killer: high blood pressure. Hypertensive Retinopathy is a condition where chronically high blood pressure damages the delicate blood vessels in the retina. Because the eyes are the only place in the body where doctors can see your blood vessels directly without surgery, your retina acts as a window into your overall vascular health.
The scary part is that you might feel completely fine while your eyes are taking a hit. In fact, most people with early-stage damage report zero visual symptoms. By the time you notice blurring or spots, the damage is often significant. But here is the good news: catching this early and getting your blood pressure under control can stop the progression and, in some cases, reverse the damage.
The Four Stages of Retinal Damage
Doctors use a standard system called the Keith-Wagener-Barker (KWB) classification is a clinical grading system used to categorize the severity of hypertensive retinopathy based on retinal appearance to figure out how far the disease has progressed. Understanding these stages helps you see why a "simple" blood pressure spike is actually a systemic emergency.
- Grade 1: This is the mildest form. The small arteries in your eye begin to narrow. You won't notice any vision changes, but a doctor using a fundoscope can see the vessels are about 15-25% thinner than they should be.
- Grade 2: Narrowing becomes more pronounced. You'll see "arteriovenous nicking," which happens when a thickened artery compresses a vein, creating a sharp bend or "nick" in the vessel.
- Grade 3: This is where things get serious. The blood-retinal barrier breaks down, leading to leakage. Doctors find "cotton wool spots" (tiny areas of dead nerve fibers) and flame-shaped hemorrhages. At this point, you're much more likely to experience blurred vision.
- Grade 4: This is the emergency zone, often linked to malignant hypertension. It includes all previous signs plus papilledema, which is swelling of the optic disc. This stage is a massive red flag for an imminent stroke.
| Stage (KWB) | Key Retinal Findings | Typical Blood Pressure | Visual Symptoms |
|---|---|---|---|
| Grade 1 | Mild arteriolar narrowing | 140/90 mmHg+ | None |
| Grade 2 | AV nicking, severe narrowing | 160/100 mmHg+ | Rare/Mild |
| Grade 3 | Hemorrhages, cotton wool spots | 180/110 mmHg+ | Blurred vision |
| Grade 4 | Optic disc swelling (Papilledema) | >180/120 mmHg | Sudden vision loss |
Why Blood Pressure Ruins Your Vision
Your retina is essentially a thin layer of light-sensitive tissue at the back of the eye, and it is incredibly hungry for oxygen. To get that oxygen, it relies on a dense network of tiny capillaries. When you have hypertensive retinopathy, your systemic blood pressure forces these vessel walls to thicken and harden to withstand the pressure. This process, known as arteriosclerosis, narrows the opening of the vessel, starving the retina of blood.
When the pressure gets too high, the vessels don't just narrow-they leak. Lipids and fluids seep into the retinal tissue, creating "hard exudates." If the pressure spikes suddenly (a hypertensive crisis), the vessels can actually burst, leading to the flame-shaped hemorrhages typical of Grade 3 and 4. This isn't just an eye problem; it's a sign that the vessels in your kidneys and brain are likely suffering similar stress.

Spotting the Warning Signs
While Grade 1 and 2 often have no symptoms, you shouldn't ignore subtle changes. If you have a history of hypertension, keep an eye out for these red flags:
- Blurred Vision: Not the usual "I need new glasses" blur, but a general haziness that doesn't go away with blinking.
- Dark Spots (Scotomas): Seeing small, floating dark spots or "holes" in your vision, especially after a significant blood pressure spike.
- Double Vision: This often accompanies severe headaches during a hypertensive emergency.
- The "Curtain" Effect: A sudden loss of a portion of your visual field, which can indicate acute retinal damage or a vascular event.
Many patients delay seeking help until their daily activities are affected. In some clinical studies, the average diagnosis happens 18 to 24 months after symptoms first appear. Don't wait for a "curtain" to fall over your vision before booking an appointment.
Modern Diagnosis: Beyond the Eye Chart
A standard vision test (reading letters on a wall) will not detect this condition. You need a dilated eye exam. Today, ophthalmologists use Optical Coherence Tomography (OCT) is a non-invasive imaging test that uses light waves to take cross-section pictures of the retina to see the thickness of the retinal layers. In exudative phases, OCT can show a thickness increase of 10-15%, helping doctors catch leakage before it causes permanent blindness.
We're also seeing a huge shift toward AI. Tools like RetinaCheck AI now allow for automated grading of retinopathy, improving diagnosis accuracy from around 75% to over 92%. This means your primary care doctor might soon be able to screen for retinal damage using an AI-assisted camera during a routine checkup, rather than sending you to a specialist for every minor concern.
How to Stop and Reverse the Damage
The most critical thing to understand is that the eye cannot be "fixed" with drops or surgery if the underlying cause is blood pressure. The only way to save your sight is to manage your systemic health. Reducing systolic blood pressure by just 25 mmHg within the first 48 hours of a crisis can resolve acute retinal changes in 65% of cases.
If you're managing high blood pressure, here's a practical approach to eye health:
- Annual Dilated Exams: If you have stable Grade 1-2 retinopathy, a yearly check is usually enough.
- Six-Month Screens: If you have "resistant hypertension" (meaning your BP stays above 140/90 despite taking three different meds), the American Heart Association now recommends screenings every six months.
- Medication Adherence: Interestingly, some data suggests ACE inhibitors are a class of medication used to lower blood pressure by relaxing blood vessels may reduce the progression of retinal damage by 32% more effectively than calcium channel blockers. Talk to your doctor about which medication is best for your specific vascular profile.
- Home Monitoring: Spend 2-3 weeks practicing consistent home BP monitoring. Understanding your spikes helps your eye doctor determine if your vision changes are acute or chronic.
Recovery timelines vary. Once blood pressure is stabilized, vision often begins to improve within 7 to 10 days. However, if you've suffered macular damage (damage to the center of the retina), it can take 3 to 6 months for partial recovery. Sadly, about 22% of patients experience permanent visual field defects even with perfect management, which is why early detection is everything.
Can I reverse the vision loss from high blood pressure?
It depends on the stage. Early changes like vessel narrowing can stabilize, and fluid leakage (edema) can often be reduced by lowering blood pressure, leading to vision improvement within a week or two. However, if the high blood pressure caused permanent nerve death (cotton wool spots) or severe scarring, that part of the vision loss is usually permanent.
Does my blood pressure have to be very high to damage my eyes?
Not necessarily. While "malignant hypertension" (above 180/120) causes rapid, severe damage, even "mild hypertension" (systolic 130-139 mmHg) can damage retinal vessels if it remains untreated for 10 years or more. Consistency of pressure matters as much as the peak height.
What is the difference between this and diabetic retinopathy?
Both involve blood vessel damage in the eye, but the mechanisms differ. Diabetic retinopathy is caused by high blood sugar damaging the vessel walls. Hypertensive retinopathy is caused by mechanical pressure. However, if you have both diabetes and hypertension, your risk of permanent vision loss is 4.7 times higher than if you had just one of these conditions.
Can an eye doctor tell if I have high blood pressure?
Yes. Because they can see the arteries and veins directly, an ophthalmologist can often spot Grade 1 changes (narrowing) at blood pressure levels as low as 140/90 mmHg. This is why eye exams are often the first place systemic hypertension is discovered.
What is papilledema and why is it a crisis?
Papilledema is the swelling of the optic disc, which happens when diastolic blood pressure typically exceeds 120 mmHg. It indicates that the pressure in your brain and eyes is dangerously high, and it is strongly associated with a much higher risk of stroke and organ failure.
Srikanth Makineni
April 9, 2026 AT 06:25standard vision tests are basically useless for this
Timothy Burroughs
April 10, 2026 AT 08:33imagine thinking your local clinic can handle this without the best american tech just pathetic honestly
these stages are just a roadmap to a stroke if you dont take it seriously
absolute madness that people ignore their bp until they go blind
Jay Vernon
April 10, 2026 AT 21:26Wow this is really scary stuff! 😱 Thanks for sharing this info. Definitely going to make sure my family gets their checkups 👁️❤️
Toby Sirois
April 11, 2026 AT 23:23Everyone knows that if you actually cared about your health you would have bought a home monitor years ago. It is honestly embarrassing that people wait for a doctor to tell them their eyes are leaking. I have been tracking my systolic for a decade and it is the only way to actually survive. Most of you just ignore the signs and then act shocked when the curtain falls. You cannot just take a pill and hope for the best. You need a full lifestyle overhaul or you are just waiting for the inevitable. It is basic biology and yet people treat it like a mystery. Stop pretending that a yearly exam is enough when your pressure is already spiking daily. Get a grip on your habits before you end up as a statistic in one of these studies. Seriously just do the work and stop making excuses for why you are not monitoring your vessels
Jitesh Mohun
April 12, 2026 AT 15:02get your meds right and stop complaining
ace inhibitors are the way to go if you actually want to save your sight
stop ignoring the 140 90 mark its a warning not a suggestion
Nikhil Bhatia
April 12, 2026 AT 19:40too much reading for a basic bp warning
Brady Davis
April 14, 2026 AT 19:38Oh sure, just a tiny bit of optic disc swelling, no big deal, only a massive red flag for a stroke! 🙄 My life is just a thrilling rollercoaster of vascular emergencies apparently
Dhriti Chhabra
April 16, 2026 AT 02:46It is most certainly prudent to emphasize the synergy between ophthalmological care and primary cardiology. One must maintain a rigorous schedule of dilated examinations to ensure the preservation of one's visual acuity over the long term.